Grand Valley Local Schools Activity and Rest-Break Guidelines for Extreme Heat

Preseason
Understanding the environmental conditions is critical to our preparation. We can prevent potential problems by following the OHSAA preseason heat acclimatization guidelines for organized sports in hot and humid weather conditions. Additionally, following adaptable guidelines based on the type of activity and the wet bulb globe temperature (WBGT) is just as important, and these are included in the OHSAA guidelines.
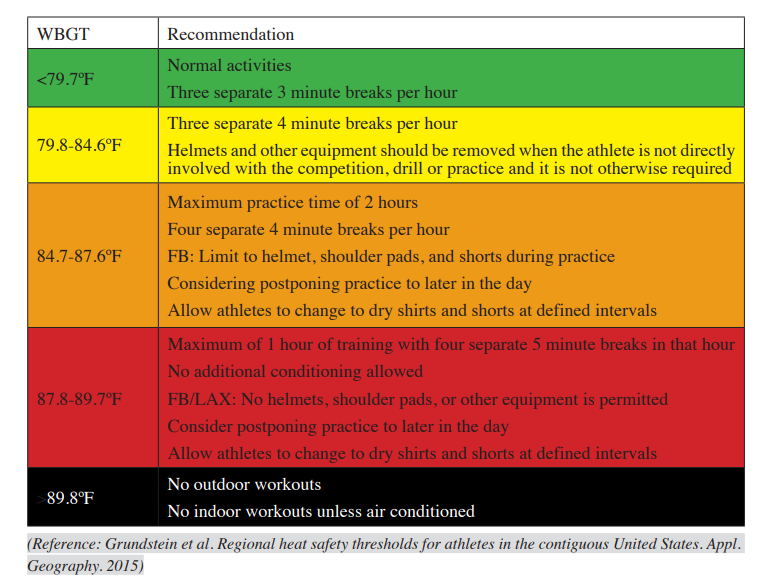
In stressful environmental conditions (see Figure 1), particularly during the first 2–3 weeks of preseason practice and scrimmages, activity should be delayed or rescheduled or the practice session shortened to reduce the risk to participants. Particular attention should be given to practice drills involving high-intensity activity and full protective equipment worn by players, as these factors may exacerbate the body's heat stress.
Turf
Synthetic turf can reach temperatures 40-70 degrees hotter than the surrounding air during scorching temperatures. It has been recorded at temperatures ranging from 120-180 degrees Fahrenheit, which significantly increases the risk of heat-related illness (dehydration, heat stress, or heat stroke), especially in children, because their bodies are less adaptable to regulating internal body temperature (Position Statement on the Use of Artificial Turf Surfaces, 2023).
Wet Bulb Globe Temperature
As responsible Athletic Trainers and Coaches, it's crucial to regularly test the air with a wet bulb globe and temperature index (WBGT index). This index, indicated in Figure 1, combines the effects of temperature, humidity, radiant heat, and airflow and should be monitored every 30 minutes during practice to adjust the intensity of practice accordingly. If the index exceeds 89.8°, outdoor workouts should be avoided, and indoor practice should be air-conditioned. Just below that, football practices can limit the wearing of equipment. Remember, your vigilance in this matter is vital to ensuring the safety of your students and preventing heat-related illnesses. While using a physical WBGT measuring device is strongly recommended for a more accurate measure of the designated location, the Zelus app can be a good resource for athletic trainers and coaches (Sports Medicine, 2023).
Figure 1
Wet Bulb Globe Temperature Guidelines
OHSAA Guidelines
https://ohsaaweb.blob.core.windows.net/files/BulletinBoard/20230822AdministratorUpdate.pdf
Click on the hyperlink under the Heat Acclimatization and Exertional Heat Illness Prevention section. Information is on Page 5 of 7 for the Sports Medicine document.
Guidelines for hydration and rest breaks
Rest breaks should involve unlimited hydration intake (water or electrolyte drinks) and rest without activity.
Helmets will be removed during rest breaks.
The site for rest time should be a "cooling zone" and not in direct sunlight (if possible) when the WBGT reading is more significant than 86F:
Preventative strategies for cooling:
Consider using ice towels or sponges and spray bottles filled with ice water, which should be available in the "cooling zone" to aid the cooling process.
Cold water immersion tubs must be available for practices to benefit any player showing early signs of heat illness.
Communication with Athletes
It is essential to inform athletes that there are several factors they can do to help mitigate dehydration and heat-related illness:
· Adequate sleep
· Hydrate before, during, and after the activity.
· Consume hydrating foods- fruits and vegetables.
· Weight checks before and after practice to identify how much fluid needs to be replaced.
· Salty sweaters need to replace sodium. Sports drinks and salty foods are the best way to replenish lost sodium.
· Avoid participation if sick. Athletes currently or recently ill may be at greater risk for exertional heat illness because of fever, dehydration, or medications (decongestants or antidiarrheal agents) (Casa et al., 2015).
· Medications that adversely affect thermoregulation include stimulants (pre-workout), antihistamines, anticholinergics (Tylenol PM), and antipsychotics. Adherence to the acclimation period is important for these athletes.
· Avoid wearing clothing that is dark, bulky, and nonbreathable material.
· Even in similar workout conditions, athletes with higher body fat percentages can dehydrate and overheat faster than those with lower percentages.
References
Casa, D. J., DeMartini, J. K., Bergeron, M. F., Csillan, D., Eichner, E., Lopez, R. M., Ferrara, M. S., Miller, K. C., O'Connor, F., Sawka, M. N., & Yeargin, S. W. (2015). National athletic trainers' association position statement: Exertional heat illnesses. Journal of Athletic Training, 50(9), 986–1000. https://doi.org/10.4085/1062-6050-50.9.07
Position statement on the use of artificial turf surfaces. (2023, November 30). Children's Environmental Health Center Department of Environmental Medicine and Public Health. Retrieved June 20, 2024, from https://mountsinaiexposomics.org/position-statement-on-the-use-of-artificial-turf-surfaces/
Sports medicine. (2023, August 1). Ohio High School Athletic Association. Retrieved June 20, 2024, from https://ohsaaweb.blob.core.windows.net/files/BulletinBoard/20230822AdministratorUpdate.pdf
Article by Denise Fisher, Certified and Licensed Athletic Trainer for University Hospitals
AEDin3 Challenge
The AEDin3 challenge, a groundbreaking initiative by University Hospitals, showcases an individual's ability to swiftly retrieve the AED, apply pads, and administer the first shock within 3 minutes. This challenge is not just about raising awareness, but about empowering you to bridge potential gaps in your Emergency Action Plan (EAP). It's about being prepared, whether it's understanding the need for a key card to enter the building or simply knowing the location of the nearest AED to the emergency.
Our commitment to the 'Anyone Can Save a Life' EAP extends to the AEDin3 Challenge, where we stress the importance of accessing an AED within 3 minutes. In the previous fall season, we made a significant discovery: student-athletes must be familiar with the locations and appearances of AEDs. This revelation underscores the necessity of planning, learning, and practicing emergency action plans with our student-athletes.
In addition to practicing the EAP and AEDin3 Challenge with the student-athletes, the coaches and I took part in an AEDin3 program created by Dr. Robert Flannery so that Grand Valley High School could apply for free AEDs. Dr. Flannery of University Hospitals recognized that many schools may not have AEDs accessible to student-athletes within 3 minutes during practices and sporting events. It's important to note that when an AED is delivered within 3-5 min to increase the survival rate. Every minute there is a delay, the survival rate drops by 10%. As the coaches and I practiced the AEDin3 Challenge (Spring of 2023) at different locations on Grand Valley's campus, we noted some shortfalls where an AED was further than 3 minutes away. The shortfalls occurred at various places on the cross-country course, the far end of the football practice field, and the community park in Orwell, where the soccer team practices and occasionally competes. Due to the shortfalls, Grand Valley qualified for three free AEDs. We have received two free AEDs so far, thanks to the AEDin3 Challenge and the coach's support. Frank Hall, athletic director, will decide how the two AEDs will be available: permanent wall location or portable AED with coaches.

University Hospitals AEDin3 Challenge Qualifiers
We extend our heartfelt gratitude to Dr. Flannery and our esteemed donors and partners, the Cleveland Browns, MTKYN Foundation, Kaulig Companies, and Stryker Medical Devices, for their unwavering support of the AEDin3 program. Your contributions have not only made a significant difference in our emergency preparedness but also underscored the importance of community collaboration in ensuring the safety of our student-athletes.
15 Northeast Ohio Schools Receive the First Cardiac Defibrillators as Part of UH AEDin3 Program
Article by Denise Fisher, Certified and Licensed Athletic Trainer for University Hospitals


Optimal OH Squat Mechanics

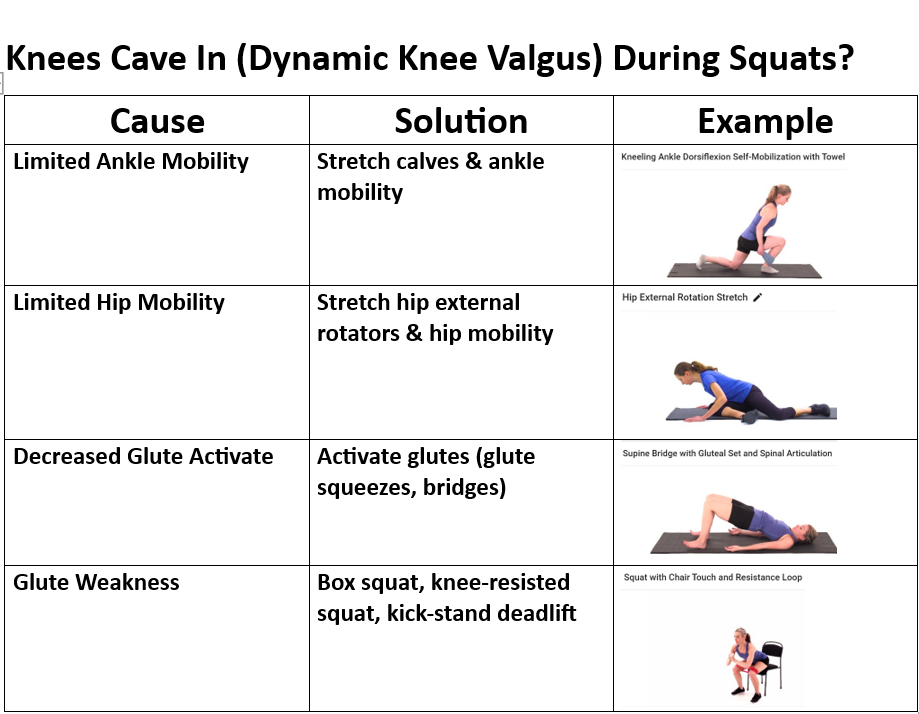
Dynamic Knee Valgus

Feet Turned Out Compensation


Emergency Action Plan
How does Grand Valley High School prepare for sports emergencies involving the student-athlete?
At the beginning of the sports season, the coaches and I plan a time to review the emergency action plan with the student-athletes. I use a program called Anyone Can Save a Life http://www.anyonecansavealife.org/ developed by the Minnesota State High School League. The reason why I chose this program is that it has easy-to-follow steps that involve the athletic trainer, coaches, and student-athletes to prepare them for immediate action to respond to life-threatening emergencies with simple steps:
1. Calling 911 to alert the Emergency Medical System (EMS)
2. Early cardiopulmonary resuscitation (CPR)
3. Early use of an automated external defibrillator (AED)
4. Early transition to EMS
The program assigns the coaches and student-athletes into teams; each team is vital in responding to emergencies. For example, Team 1 is the 911 team. Team 1 will review the following questions on what they need to know. Where is the closest cell phone or landline? What is the school's address, and where is the emergency located on GV's campus? What is the best access point for the ambulance to arrive for both practice and events? The next step for Team 1 is to assign the team their roles, such as having two students call 911, two more students meet the ambulance at the access point, and lastly, two more students locate the athletic trainer and athletic director.
A team approach is needed to respond to an emergency to avoid panic and confusion. So, why would we involve a student-athlete when adults are present? First, there are times when only one coach is conducting the practice, and what happens when it is the coach who is having an emergency? That is why I feel it is essential to empower student-athletes to know how to respond to an emergency without panic or confusion. Educating the student-athlete may also help them in their personal lives should they face a life-threatening emergency with a loved one, friend, or a witness to someone in need.
AEDin3 Challenge
The AEDin3 challenge is a new initiative by University Hospitals that demonstrates the capability of a person to get the AED, apply pads, and deliver the first shock in under 3 minutes. The challenge is to bring awareness to the importance of detailed preparation and potential gaps in the EAP, such as needing a key card to enter the building or simply knowing the location of the nearest AED to the emergency.
When we practice the EAP "Anyone Can Save a Life," I also review in detail and practice the AEDin3 challenge and the importance of having access to an AED in less than 3 minutes. What I have learned this past fall season is that many of the student-athletes needed to understand where the AEDs are located and what they look like. That was an ah-ha moment for many and illustrated the importance of planning, learning, and practicing emergency action plans.
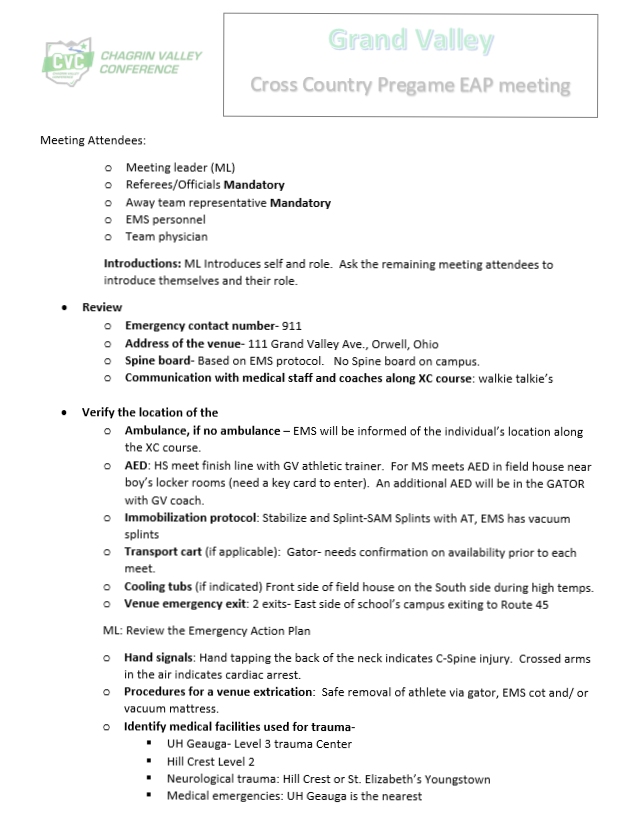
Pregame EAP Meeting
In addition to the EAP training with GV's student-athletes, the CVC started a mandatory Pregame Emergency Action Plan Meeting with coaches, officials, and athletic trainers before all sporting contests. OHSAA may also make the Pregame Emergency Action Plan Meeting a state-wide initiative. Figure 1 is an example of the EAP meeting for XC Meets.
Figure 1
CVC Pregame EAP Meeting

Corrective Exercise Benefits on Inactive Youths

The implementation and commitment to a corrective exercise program would provide a way to offset the negative impacts on our society before the development of medical conditions. Nowadays, chronic physical inactivity in youths will exhibit habitual nonfunctional living characteristics that transpire to poor postural adaptations from their sedentary lifestyle (Fahmy, 2022), leading to high incidences of obesity, poor motor skills, and musculoskeletal disorder weakness (Liao et al., 2019). Over time poor postural adaptations will lead to musculoskeletal dysfunctions from imbalances in muscle recruitment and length between muscles that stabilize joints and muscles that mobilize joints (Comerford & Mottram, 2001). Youths may feel discouraged from traditional physical activity in the presence of a musculoskeletal dysfunction because it may not feel good to exercise, or they lack confidence and motivation, thus retreating to their sedentary lifestyle. A corrective exercise program is a safe and individualized program that identifies neuromusculoskeletal dysfunction, followed by developing an action plan and integrative exercise techniques (Fahmy, 2022). A corrective exercise program will also address the youth's environment and goals, which are essential to the program's success and the continued support of adopting a positive and healthy lifestyle (Fahmy, 2022).
Walker et al. (2018) medical report identified physical inactivity in youths as an exercise deficit disorder. The medical report examined a three-tiered strategy for preventing pediatric physical inactivity by improving the quality of life and decreasing morbidity and economic burden (Walker et al., 2018). The first tiered strategy is tertiary prevention, providing treatment for health complications from an existing disease (Walker et al., 2018). Tertiary care is the current health care model for the USA; however, in the past, before the twentieth century, the health care model focused on preventing diseases (Walker et al., 2018).
The second and third-tiered strategies are elements discussed in corrective exercise programs: early treatment and immunization against exercise deficit disorder (Walker et al., 2018). Early treatment and immunization of this disorder begin with engaging youths lacking physical activity (Walker et al., 2018). When early physical activity is promoted, youths will demonstrate improved health parameters (Walker et al., 2018). According to Walker et al. (2018), identifying and treating muscle strength and motor skills deficiencies are necessary for developing a solid foundation to carry through to later stages of development (Walker et al., 2018). A corrective exercise program would aim to address these deficiencies through the corrective exercise continuum objectives (Fahmy, 2022).
In conclusion, corrective exercise programs are valuable to this population's health and well-being. The benefits to society are considerable by applying safe and effective means of improving one's overall health and well-being from exercise.
If you are a parent of a child (athlete or non-athlete) at Grand Valley MS and HS (ages 12-18) and are interested in a free Corrective Exercise Consult, please contact me at denise.fisher@grandvalley.school. The free consult will include health history, movement analysis, education on findings of the movement analysis, and 1st phase of the corrective exercise plan. The consult generally takes about 45-60 minutes. Please note that a medical clearance may be required depending on the discoveries in the health history.
Article by Denise Fisher 6/14/2023
Certified and Licensed Athletic Trainer
Corrective Exercise Specialist
References
Comerford, M., & Mottram, S. (2001). Movement and stability dysfunction – contemporary developments. Manual Therapy, 6(1), 15–26. https://doi.org/10.1054/math.2000.0388
Fahmy, R. (Ed.). (2022). NASM Essentials of corrective exercise training (2nd ed.). Jones & Bartlett Learning.
Liao, T., Li, L., & Wang, Y. (2019). Effects of functional strength training program on movement quality and fitness performance among girls aged 12–13 years. Journal of Strength and Conditioning Research, 33(6), 1534–1541. https://doi.org/10.1519/jsc.0000000000002190
National center for chronic disease prevention and health promotion. (2022, April 27). CDC Centers for disease control and prevention. Retrieved May 12, 2022, from https://www.cdc.gov/chronicdisease/resources/publications/factsheets/physical-activity.htm
Walker, G., Stracciolini, A., Faigenbaum, A. D., & Myer, G. D. (2018). Physical inactivity in youth. ACSM's Health & Fitness Journal, 22(2), 42–46. https://doi.org/10.1249/fit.0000000000000370

Six Pack Abs
What is the best exercise for the core?
There are many excellent exercises that strengthen the abdominal muscles; however, I feel this can be seen as a controversial topic because there is so much misinformation out there, especially for the public. I admit that I used to only strengthen my abdominal muscles with full sit-ups, Roman chair leg lifts, and crunches when I was younger. It wasn’t until I went through yoga instructor training in my early 20s that I learned better ways to strengthen my abdominal muscles. However, I do feel the above exercises have a place in strength and conditioning programs, but I don’t think they are as optimal as I once thought. Brookbush (2016) did deflate my belief when he explained there is no such thing as the lower abdominals. It makes sense because you typically can not separate the action into upper or lower contractions when you tighten or draw in your abdomen. This goes back to knowing and understanding your anatomy well. Brookbush (2016) explained this based on studies that looked at the movement and stabilization of the spine, hips, and pelvis, noting that the rectus abdominis is recruited as one muscle unit. There is one caveat to the rectus abdominis as a one-unit muscle; the stomach roll in belly dancing is noted in one study to result in deliberate and separate recruitment of the upper and lower rectus abdominis muscles (Brookbush, 2016).
It is hard for me to identify one specific exercise that best strengthens the abdominal muscles because additional factors like physical ability, balance, mobility, and age need to be considered. Since I work with high school athletes, I must be cautious about my exercise selection because they may lack the strength and stability to perform certain abdominal exercises correctly. The exercise I have selected as the best abdominal exercise is the plank. This selection has several reasons: easy to modify, progressional, and can be done with or without equipment. I also like the plank because it is a foundational exercise that works the entire body and helps athletes transition safely to Olympic lifts by understanding core activation. The research by Snarr & Esco (2014) looked at the variations in rectus abdominis, external obliques, and erector spinae raw muscular activity and the percentage of a maximum voluntary contraction between a traditional plank and a plank with instability devices. The study used electromyography (EMG) to analyze maximum voluntary contraction (MVC) and electromyographic activity of the rectus abdominis, external obliques, and lumbosacral erector spinae. The subjects were instructed on the five different plank exercises: regular plank on forearms, plank with elbows and forearms on the Swiss ball (EB), plank with feet on the Swiss ball (FB), plank with elbows in TRX suspension trainer (ET), and plank with feet in TRX suspension trainer (FT). The research findings were interesting and very informative, which identified significantly greater EMG activity of the analyzed musculature when planks were performed with the Swiss ball or TRX suspension trainer. The ET produced the highest mean raw and %MVC for the rectus abdominis activation. The external obliques had the most increased EMG activity for both raw and %MVC with the FB. For the erector spinae, the highest raw EMG recording was with both EB and ET, and the highest %MVC was in the ET plank. This doesn’t mean planks with instability devices are superior to regular plank exercise. The traditional plank provides sufficient abdominal musculature activation to increase strength and stability (Snarr & Esco, 2014). The variation of the EMG results of the three muscles during planks with instability devices is explained by changes in the distance between the center of mass and the location of the instability device. The authors also considered the difference in EMG data between the Swiss ball and the TRX suspension trainer due to the differences in degrees of freedom.
To conclude, I consider the plank one of the best abdominal exercises because it can be modified and advanced for different skill levels. The plank also includes a total body muscle activation approach from the head to the toes allowing the individual to be consciously aware of their body alignment and isometric muscle contractions during the exercises.
Article by Denise Fisher 4/18/2023
References
Brookbush, B. (2016). Human movement science & functional anatomy of the: rectus abdominis (and pyramidalis). Brookbush institute human movement science. Retrieved December 6, 2021, from https://brookbushinstitute.com/course/rectus-abdominis-pyramidalis
Snarr, R. L., & Esco, M. R. (2014). Electromyographical comparison of plank variations performed with and without instability devices. Journal of Strength and Conditioning Research, 28(11), 3298–3305. https://doi.org/10.1519/jsc.0000000000000521
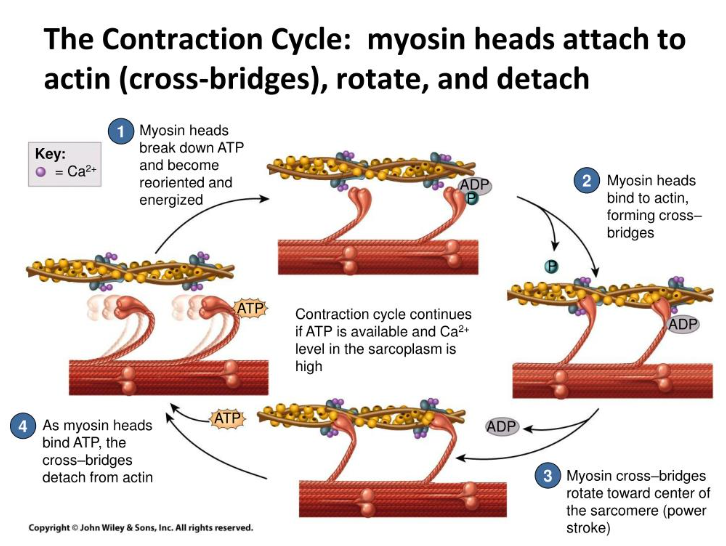
Overhead Baseball Pitch: Mechanics and Compensations that Lead to Injury
The overhead baseball pitch is an incredible demonstration of the power transmitted through the kinetic chain, generated in the lower extremity and transferred through the upper extremity (Chalmers et al., 2017). Specifically looking at the upper extremity, the overhead baseball pitch is an open kinetic chain movement (Findley & Brown, 1999). The open kinetic chain (OCK) movement does not have a fixed distal segment, enabling free movement that is not fixed to an object (Prokopy et al., 2008). It's important to note that the OKC movements can be associated with closed chain movements, which is demonstrated in the overhand baseball pitch when the forces are generated in the lower extremity before transferring up the kinetic chain to the upper extremity (Findley & Brown, 1999).
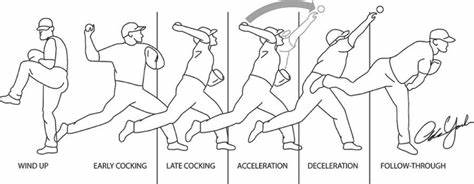
To identify the common compensations seen during the overhead pitch, one must have a general understanding of the pitching phases and how they help one to analyze muscle activity and joint actions occurring within each phase. Researchers who study the overhead pitch will use specific tools to measure kinetic, kinematics, and electromyography (EMG) during each pitch phase, allowing them to understand better what muscles are active during the phases (Escamilla & Andrews, 2009). The six phases that describe the pitching motion are wind-up, stride, arm cocking, arm acceleration, arm deceleration, and follow-through (Chalmers et al., 2017).
During the wind-up phase, the pitcher puts himself in a balanced position, which is critical for preparing force generation. Hands are together at the chest, and the lead leg is raised (Chalmers et al., 2017). Injuries are low during this phase; however, as noted by Seroyer et al. (2020), if the pitcher alters his center of gravity by initiating the movement prematurely, the force generated through the kinetic chain will be altered, resulting in significant stress at the glenohumeral and elbow joint to propel the ball forward at top speed.

The stride phase initiates the arm cocking position to generate ball velocity. The lead foot makes ground contact on the mound with the hip and knee extending while the pelvis rotates to face the batter on the home plate (Chalmers et al., 2017). During this phase, shortened stride length compensates for poor hip mobility from flexibility restrictions in the hamstring of the lead leg and stance leg hip flexors or rotators (Calabrese, 2013). Another compensation to consider is an abnormal placement of the stride foot due to decreased hip mobility, which is noted as the excessive closed foot contact position (Christoffer et al., 2019). A standard stride foot placement should be facing toward the home plate (Calabrese, 2013). The compensation occurs when the lead leg hip has overactive internal rotators and the stance foot has overactive external rotators (Calabrese, 2013). The excessive closed foot contact position will limit the lead leg and pelvis from transmitting the force to the pitching arm, which leads to timing errors and loss of proper sequence of the body and the pitching arm, causing more stress on the anterior shoulder, scapular stabilizers, and medial elbow (Christoffer et al., 2019; Calabrese, 2013). A study by Albiero et al. looked at the hip active range of motion (AROM) and pitching biomechanics during a fastball pitch in adolescent baseball pitchers. The authors hypothesized that poor active hip range of motion would decrease the energy transfer through the kinetic chain, causing subpar pitching mechanics and injury to the pitcher. The study involved twenty-one healthy adolescent baseball pitchers. The pitchers were tested by a single session that included a detailed clinical and biomechanical analysis using specialized cameras and markers. The study occurred during preseason baseball when the pitchers were already pitching twice weekly. The results indicated five significant relationships between pitching biomechanics and hip AROM flexibility. The findings confirmed the importance of having optimal hip AROM to complete normal pitching biomechanics through the kinetic chain aiding in pitch velocity and decreasing injury up the kinetic chain.

The arm cocking phase begins when the lead foot contacts the ground and finishes with maximal shoulder external rotation of the pitching arm (Calabrese, 2013). Late in this phase, significant injury can occur to the pitching arm because shoulder internal rotational torque and elbow valgus torque are at their peak (Chalmers et al., 2017). The repetitive loading leads to injuries of the superior labral anterior-posterior (SLAP) and ulnar collateral ligament (Chalmers et al., 2017). Pitchers that compensate with exaggerated shoulder horizontal abduction to increase ball velocity are at risk for anterior translation of the humeral head, which will produce internal impingement during the end of the cocking phase (Itami et al., 2018). The most common overactive muscles in the cocking phase are the teres minor, infraspinatus, and middle and posterior deltoids. The underactive scapular muscles are the upper and lower trapezius and serratus anterior muscles. The overactive and underactive muscles described above create imbalances in the pitching arm that can also be observed when the elbow is positioned below the shoulder's height during the end of the cocking phase (Calabrese, 2013).

The acceleration phase starts when the shoulder is maximally externally rotated, followed by the change to internal rotation, the extension of the elbow, and flexion of the wrist (Chalmers et al., 2017). During this phase, compensations are noted for different levels of pitchers. For example, it's not uncommon for youth and amateur pitchers to demonstrate weakness in scapular muscles and overactivity of the biceps and rotator cuff (RTC) muscles resulting in overuse injuries (Calabrese, 2013; Christoffer et al., 2019). In all levels of pitchers, maintaining stabilization of the scapula is critical for reducing the risk of shoulder impingement, RTC muscle strains, and biceps strains (Calabrese, 2013). However, according to Gowan et al. (1987, as cited in Escamilla & Andrews, 2009), professional baseball pitchers demonstrated better coordination of their kinetic chain segments, resulting in less glenohumeral instability minimizing stress to the RTC musculature and biceps.
The arm deceleration phase is the most violent in the baseball pitch because of the large forces generated at the shoulder complex to slow down the pitching arm momentum (Seroyer et al., 2010). The phase begins when the ball is released from the hand ending in maximal internal rotation of the shoulder (Escamilla & Andrews, 2009). This phase differs from the other phases because of the high compressive forces required to decelerate the arm to avoid shoulder distraction (Escamilla & Andrews, 2009). The posterior muscles are eccentrically contracting to maintain the humeral head's optimal position, while scapular muscles stabilize to reduce the forces on the RTC muscles and biceps (Calabrese, 2013). Due to the high compressive forces in the shoulder, the muscles and static stabilizers are very susceptible to overload, which is seen when a pitcher demonstrates fatigue within the kinetic chain (Itami et al., 2018). The overload will lead to scapular dyskinesia resulting in compensations at the shoulder or elbow (Itami et al., 2018). Glenohumeral internal rotation deficit is an example of a commonly discussed compensation at the shoulder from posterior capsule tightness, underactive scapular upward rotators, and retractors (Itami et al., 2018).

The last phase of the overhead baseball pitch is the follow-through. During this phase, the pitching arm moves in horizontal adduction and internal rotation as the body moves forward (Calabrese, 2013). Due to the decrease in joint loading, fewer injuries are attributed to this phase (Seroyer et al., 2010).

The best early prevention strategies to avoid future compensations noted during the overhead baseball pitch are learning the proper pitching mechanics in the beginning stages (Fortenbaugh et al., 2009) and having a balanced strength and mobilization program for the shoulder complex, trunk, and lower extremities. Another essential prevention strategy is to avoid training overuse and pitching fatigue. Fortenbaugh et al. research identified the importance of combining pitch count and kinematics/ kinetics to identify pitcher fatigue during the pitching motion more effectively. Since muscular fatigue is attributed to a high pitch count, the effects are seen later as imbalances within the shoulder and scapular muscles (Itami et al., 2018).
In closing, the overhead baseball pitch is a complex motion requiring the entire kinetic chain to work from the ground up in a systematic way to avoid injury and fatigue. In my opinion, the pitcher should be recommended to start with a strong foundation and optimal joint mobility in the upper and lower extremities and spine before learning the overhead pitching technique. Once the process is mastered, pitch volume should be determined based on the performance quality and age. Strength and endurance training programs should include open and closed kinetic chain exercises to gain the maximum benefits from both types of training. Lastly, encouraging youth athletes to avoid specialization early in their sporting careers will help decrease the risk of compensation, injuries, and burnout from year-round training.
Watch Drew Storen's pitching mechanics: Click on the link below.
Drew Storen pitching mechanics in slow motion 1000 FPS
Article by Denise Fisher 4/5/2023
References
Albiero, M. L., Kokott, W., Dziuk, C., & Cross, J. A. (2021). Relationships between hip flexibility and pitching biomechanics in adolescent baseball pitchers. Journal of Athletic Training. https://doi.org/10.4085/1062-6050-0103.21
Calabrese, G. J. (2013). Invited clinical commentary pitching mechanics, revisited. The International Journal of Sports Physical Therapy, 8(5), 660.
Chalmers, P. N., Wimmer, M. A., Verma, N. N., Cole, B. J., Romeo, A. A., Cvetanovich, G. L., & Pearl, M. L. (2017). The relationship between pitching mechanics and injury: A review of current concepts. Sports Health: A Multidisciplinary Approach, 9(3), 216–221. Retrieved October 15, 2021, from https://doi.org/10.1177/1941738116686545
Christoffer, D. J., Melugin, H. P., & Cherny, C. E. (2019). A clinician’s guide to analysis of the pitching motion. Current Reviews in Musculoskeletal Medicine, 12(2), 98–104. https://doi.org/10.1007/s12178-019-09556-4
Escamilla, R. F., & Andrews, J. R. (2009). Shoulder muscle recruitment patterns and related biomechanics during upper extremity sports. Sports Medicine, 39(7), 569–590. https://doi.org/10.2165/00007256-200939070-00004
Findley, B. W., & Brown, L. (1999). Open-versus closed-kinetic chain exercise. Strength and Conditioning Journal, 21(4), 39. Retrieved October 15, 2021, from https://doi.org/10.1519/00126548-199908000-00008
Fortenbaugh, D., Fleisig, G. S., & Andrews, J. R. (2009). Baseball pitching biomechanics in relation to injury risk and performance. Sports Health: A Multidisciplinary Approach, 1(4), 314–320. https://doi.org/10.1177/1941738109338546
Itami, Y., Mihata, T., McGarry, M. H., Lin, C. C., Patel, N. A., Kantor, A., Neo, M., & Lee, T. Q. (2018). Effect of increased scapular internal rotation on glenohumeral external rotation and elbow valgus load in the late cocking phase of throwing motion. The American Journal of Sports Medicine, 46(13), 3182–3188. https://doi.org/10.1177/0363546518800267
Seroyer, S. T., Nho, S. J., Bach, B. R., Bush-Joseph, C. A., Nicholson, G. P., & Romeo, A. A. (2010). The kinetic chain in overhand pitching: Its potential role for performance enhancement and injury prevention. Sports Health: A Multidisciplinary Approach, 2(2), 135–146. https://doi.org/10.1177/1941738110362656
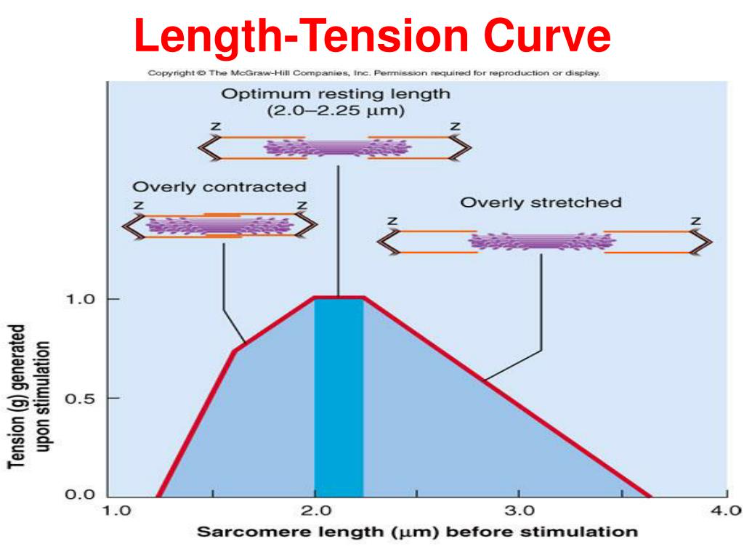
Optimal length-tension relationship of a muscle is the preferred length of the muscle at rest, which in turn allows the muscle to produce the greatest amount of force during movement because there is the ability for sufficient cross bridging of actin-myosin for more significant force generation (Fahmy, 2022). When a muscle is in a shortened and overactive state, the cross bridging of actin and myosin filaments is preestablished in a chronic condition of overlap, which restricts the muscle's ability to generate more force because filament space is limited (Fahmy, 2022). The opposing muscle position is the lengthened and underactive state, which places the actin and myosin filaments apart, thus limiting the cross bridging ability and reducing the capacity to generate force (Fahmy, 2022).
An example of an altered length-tension relationship in the body is when one side of a joint has shortened from overactive musculature resulting in the opposite side of the joint musculature being lengthened and underactive due to decreased neural drive from reciprocal inhibition (Fahmy, 2022). To visualize an altered length-tension relationship in the human musculoskeletal system would be to picture someone who has a rounded shoulder and forward head posture, also known as upper body dysfunction (Brookbush, 2013), which according to Colbert et al. (2022), is possibly due to limitations functional thoracic range of motion causing an incongruent relationship during movement between the thorax convex surface with the scapula concave surface. For more on the structural components, go to https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8811512/. Scroll down to discussion.
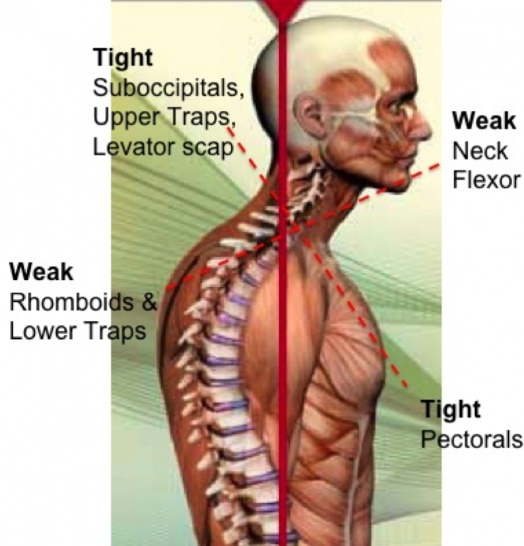
Muscles that stabilize the scapula from the thorax rely on the convex surface of the thorax to maintain an optimal length-tension relationship; such relationships are the serratus anterior, trapezius, and rhomboid (Colbert et al., 2022). Changes in the thorax from a convex to a flatter surface will affect the scapula resting position and inhibit normal movement with the thorax, therefore altering the length-tension relationship of the scapular stabilizers (Colbert et al., 2022). Additionally, muscles affected by the scapulothoracic joint changes and poor posture are the lengthened and underactive upper trapezius, scalenes, sternocleidomastoid (SCM), and rhomboid and the shortened and overactive muscle of the pectoralis major (Colbert et al., 2022). Brookbush (2013) included a detailed list of muscles considered short and overactive based on upper body postural adaptations, which include but are not limited to the pectoralis minor, levator scapulae, latissimus dorsi, teres major, and subscapularis. It's important to note that changes in upper body dysfunction that result in postural adaptations occur gradually over time (Brookbush, 2013). Arthokinematic changes from upper body dysfunctions will eventually lead to mechanical restrictions that will result in greater modifications when compared to soft tissue restrictions alone (Brookbush, 2013).
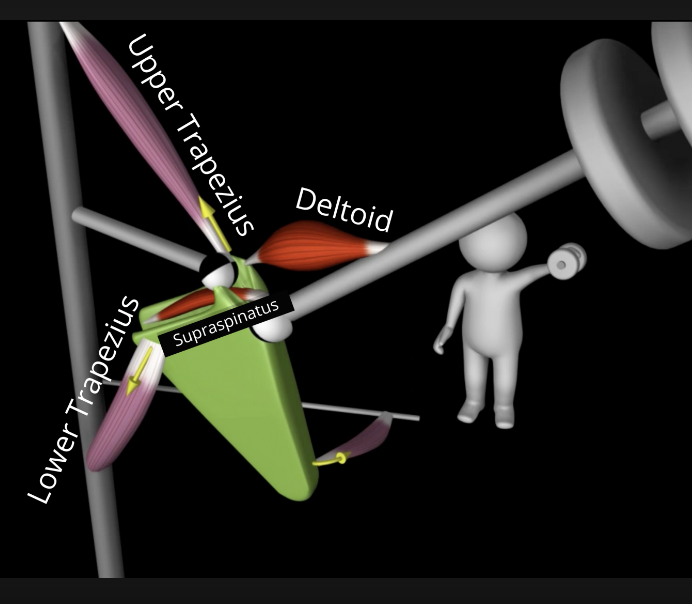
The scapula, in my opinion, is largely a balance of muscles that create force-coupling relationships to maintain adequate alignment of the scapula position with the thorax and shoulder. During shoulder elevation, the scapulothoracic muscles (trapezius, serratus anterior, pectoralis minor, levator scapula, and rhomboid) regulate the scapular movements (Umehara et al., 2019). For the scapula to move optimally, the trapezius and serratus anterior muscles need to function in coordination with the scapulothoracic muscles as a force-coupling relationship (Umehara et al., 2019). The force-coupling relationship between the scapulothoracic muscles is required for optimal scapular and glenohumeral movements (Umehara et al., 2019). An example of a healthy shoulder joint kinematics is elevation, upward and internal rotation, and posterior tilt of the scapula, which means the muscles are working together to maintain force-coupling relationships. When the muscles of the scapulothoracic present with an altered length-tension relationship, such as an underactive and lengthened upper and lower trapezius and serratus anterior with an overactive and shortened pectoralis minor, levator scapulae, and rhomboid the force coupling relationship is decreased, which limits the amount of group force transmitted to the scapula for movement (Umehara et al., 2019). Another way to look at it is the synergy of the muscle groups acting at the scapula is lost due to the imbalances between the muscle groups (Fahmy, 2022).
Article by Denise Fisher 4/5/2023
References
Brookbush, B. (2013). Upper body dysfunction (UBD). Brookbush institute human movement science. Retrieved May 18, 2022, from https://brookbushinstitute.com/course/upper-body-dysfunction-ubd
Colbert, L., Harrison, C., & Nuelle, C. (2022). Rehabilitation in overhead athletes with thoracic outlet syndrome. Arthroscopy, Sports Medicine, and Rehabilitation, 4(1), e181–e188. https://doi.org/10.1016/j.asmr.2021.11.007
Fahmy, R. (Ed.). (2022). NASM essentials of corrective exercise training (2nd ed.). Jones & Barlett Learning.
Umehara, J., Yagi, M., Hirono, T., Komamura, T., Nishishita, S., & Ichihashi, N. (2019). Relationship between scapular initial position and scapular movement during dynamic motions. PLOS ONE, 14(12), e0227313. https://doi.org/10.1371/journal.pone.0227313
Part 1: Basic Mechanics of the Back Squat
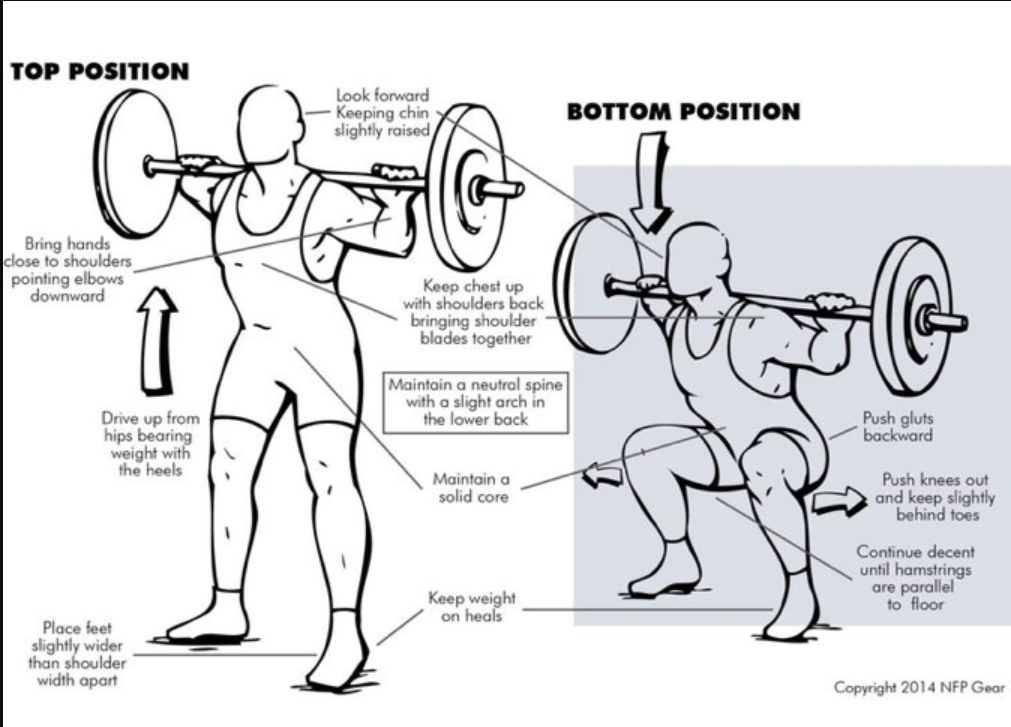
The back squat is a fundamental exercise used in our daily lives and during most resistance training programs; however, it is typically done incorrectly. Squat biomechanics may seem easy, yet it is a complex movement that requires our muscles to coordinate by activating and firing jointly to achieve proper movement patterns. With regard to performance, the back squat is used to improve strength and performance and decrease the risk of injury (Swinton et al., 2012). One such way the back squat reduces injury is by minimizing anterior displacement of the knee (Swinton et al., 2012), which lowers the risk of anterior cruciate ligament (ACL) tears. However, this is only achievable if the squat is done correctly. The figure below is an excellent illustration of what is required to achieve an ideal back squat. Now, it's important to note that there are squat variations, and the image of the back squat below is just an example of the significant components one should achieve while performing the back squat. One feature that was not illustrated and is essential to perform at the feet is to try "spreading the floor underneath your feet." This component should be done throughout the squat movement; the individual will feel more stable when done correctly.
Back Squat Positioning and Additional Considerations
No-heeled shoes. Preferably flat-sole tennis shoes or go without shoes. Heeled shoes make the back squat quadricep-dominant. Quadricep dominant exercises increase ACL loading and anterior shear force.
Stance position will depend on the individual's goals but is primarily related to one's femoral length (thigh bone). A long femoral length requires a wider stance, while a short one needs a more narrow stance. It's also important to understand that an externally rotated foot position will engage the quadriceps more, and a neutral (straight) foot position will engage the tensor fascia lata, IT band, and gluteus medius.
Look slightly upwards the entire time—chest up.
Squeeze shoulder blades and point elbows down.
Spread the floor underneath your feet. Try to tear the floor with your feet.
Lead with the glutes (butt) 1 inch: push the butt back without leaning forward.
Push out with your knees and go down as far as possible.
These considerations aim to spread the pressure out over the entire body. Avoid making one muscle group do all the work, leading to injury.
Figure 1: Back Squat Mechanics
References
Swinton, P. A., Lloyd, R., Keogh, J. L., Agouris, I., & Stewart, A. D. (2012). A biomechanical comparison of the traditional squat, powerlifting squat, and box squat. Journal of Strength and Conditioning Research, 26(7), 1805–1816. https://doi.org/10.1519/jsc.0b013e3182577067
Article by Denise Fisher 3/23/2023

What is the best type of strength training for swimmers?
Before answering this question, I would like to explain the difference between open and closed kinetic training.
The benefits of open and closed kinetic training regarding the shoulder complex are important to understand when developing a strength program because they will allow one to decide the program's focus: correcting specific imbalances versus increasing global strength and stability. For instance, open kinetic chain (OKC) exercises stimulate muscles in isolation, and closed kinetic chain (CKC) exercises stimulate muscles by co-activating surrounding muscle groups. OKC does not have a fixed distal segment, enabling free movement that is not fixed to an object (Prokopy et al., 2008). Muscle activation is also customarily proximal to the distal segment, and the distal part is usually the hands or feet. An example of an OKC is standing cable rows. CKC has a fixed distal segment when met with resistance (Prokopy et al., 2008). An example of a CKC is floor push-ups. In CKC exercises, the extremity muscle activation is sequential from distal to proximal.
For swimmers, dryland strength training will be composed of open and closed kinetic chain exercises. Upper extremity OKC exercises allow a swimmer to strengthen underworked muscles aiding in injury prevention. A great example in swimmers is strengthening the weak external rotators (ER) because the internal rotators (IR) become overdeveloped from the repetitive front crawl technique. The OKC exercises are also beneficial for strengthening the scapular muscles and correcting imbalances. In contrast, the CKC exercises target both agonist and antagonist muscle groups and greater joint stability, significantly increasing strength around the shoulder complex, which reduces the risk of injury during CKC exercises (Moradi Shahpar et al., 2019).
Shahpar et al. (2019) studied the response of an eight-week open and closed dryland training program on muscle torque of the internal and external shoulder rotators in swimmers. Participants in the study were forty-five healthy male swimmers between the ages of 18-25. The swimmers were divided into the OKC group, the CKC group, and a control group. Except for the control group, each performed its prescribed exercises three times a week for eight weeks. Pre and post-measurements of peak torque of the internal and external shoulder rotators were completed using the isokinetic HUMAC NORM machine at various speeds of 60, 120, and 180 degrees. The study's results demonstrated improvements in both internal and external shoulder rotator torque. However, there was a substantial difference between open and closed kinetic training, with open kinetic training showing more significant improvements in enhancing internal and external shoulder torque.
Both forms of training have a purpose in injury prevention, rehabilitation, and strength programs. The focus of dryland programs should include anterior and posterior muscle balancing, muscle endurance, strength building, improvement of joint stability, and neuromuscular control, which is addressed when including both OKC and CKC exercises (Moradi Shahpar et al., 2019). If the individual only did OKC exercises, they would lose out on the benefits of CKC, which increase proprioception, joint stability, and overall strength gains of surrounding muscles (Moradi Shahpar et al., 2019).
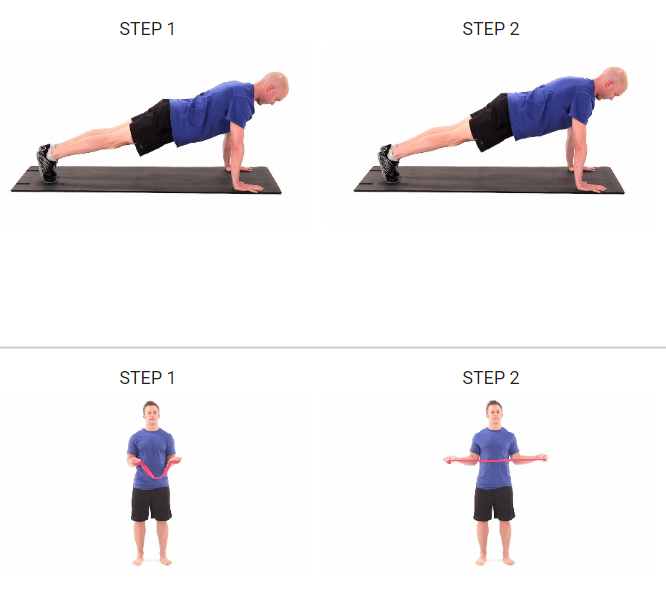
Examples of a closed kinetic chain push-up plus exercise and an open kinetic chain shoulder external rotation exercise with a theraband. Images are from Medbridge.
Article by Denise Fisher
References
Moradi Shahpar, F., Rahnama, N., & Salehi, S. (2019). The effect of 8 weeks of open and closed kinetic chain strength training on the torque of the external and internal shoulder rotator muscles in elite swimmers. Asian Journal of Sports Medicine, 10(2). https://doi.org/10.5812/asjsm.82158
Prokopy, M. P., Ingersoll, C. D., Nordenschild, E., Katch, F. I., Gaesser, G. A., & Weltman, A. (2008). Closed-kinetic chain upper-body training improves the throwing performance of NCAA division I softball players. Journal of Strength and Conditioning Research, 22(6), 1790–1798. https://doi.org/10.1519/jsc.0b013e318185f637
Considerations for Increasing Muscle Mass with Nutritional Supplementation
THIS INFORMATION IS FOR EDUCATIONAL PURPOSES ONLY. FOR MORE INFORMATION, PLEASE WORK WITH A REGISTERED SPORTS DIETICIAN.
Increasing Muscle Mass
My first suggestion for an athlete would be to focus on their diet and make quality choices. I would encourage the athlete to establish an ideal and reasonable nutrition plan that provides adequate caloric intake and appropriate food consumption with timing (See Figure 2) to support their needs and improve their performance, strength, and power, which most likely will require assistance from a sports dietician. Andersen et al. (2005) research showed positive results in muscle hypertrophy of type I and II muscle fibers when young, physically active adult males consumed two servings of 25 grams of protein immediately before and after resistance training for 14 weeks at three times a week. Andersen et al. (2005) suggest that the mechanism for the increase in muscle hypertrophy is due to a positive protein balance, which means the rate of protein synthesis was more significant than protein breakdown.
Morton et al. (2017) conducted a systematic review of the effect on skeletal muscle from different levels of protein intake, which indicated that an increase in the ingestion of protein at 0.5 and 3.5 g/kg/day was associated with increased muscle mass and this was shown to occur with and without weight training. Research has also established that adding protein with a higher amount of the amino acid leucine could help provide a more remarkable environment for muscle protein synthesis (Smith-Ryan & Jose, 2013). Foods high in leucine are chicken breast, lean beef, and greek yogurt (Jeukendrup & Gleeson, 2019). So, with that said, it is safe to say that food should always come first before considering supplements. However, other influences must be considered, such as age, genetics, lifestyle characteristics (sleep and stress management), and current and past training history. All these components and one's daily nutrition will play a role in their success and ability to attain performance goals.
Supplement Regimen
I frequently get questions about multivitamins, "Mega" multivitamins, Creatine, and Whey protein supplements, so here is what I know:
First, "mega" multivitamin supplements do not help increase muscle mass, strength, and power. Taking a "mega" multivitamin/mineral supplement may also fall into the category of unsafe supplementation and is not needed when an individual is consuming a well-round whole foods diet with ideal amounts of macro and micronutrients. The added expense of buying a "mega" multivitamin could go towards purchasing high-quality foods; however, there are times when recommended dietary allowance (RDA) multivitamin may have a purpose that is important for specific stages in life or those that struggle with nutritional challenges (Garthe & Maughan, 2018). For instance, vegans or athletes with a particular medical condition may require medical guidance on multivitamins (Garthe & Maughan, 2018). One may also want to consume an RDA multivitamin as an insurance policy to benefit their overall health if they lack adequate intake for the day.
Figure 1 below illustrates how athletes should manage their nutritional development through the years.
Whey Protein
Whey protein would be a good supplement for athletes, pending they are getting most of their calories and protein from quality food sources. However, supplementing with whey protein may be helpful when it is hard to ingest the required amount of protein through food alone or simply for convenience. Smith-Ryan & Jose (2013) reported that consuming 20-30 grams of whey protein from isolates or hydrolysates before, during, and after exercise has effectively increased anabolic activation. For instance, an athlete may consider consuming 20-25 grams of protein (food sources or whey) with each meal, which may include co-ingesting a small amount of protein with carbohydrates during exercise, followed by a post-exercise feeding of 20-25 grams and possibly another protein feeding before bed to maintain a positive protein balance for muscle protein synthesis (van Loon, 2013).
Creatine
Creatine (Cr) would be a relatively safe supplement for athletes. As stated by Smith-Ryan & Jose (2013), all humans are consumers of Cr, which supplies high-intensity, short-duration exercise, i.e., sprinting, so it is a supplement that would be appropriate for many forms of exercise. Cr can be found in foods such as beef, pork, and fish or through a powder supplement that is mixed into a liquid, and either form is highly bioavailable (Smith-Ryan & Jose, 2013).
The benefits of Cr are its effectiveness in improving lean body mass, strength, and high-intensity exercise (Kerksick et al., 2018). Additionally, and somewhat theoretically, Cr supplementation helps to increase its storage in the skeletal muscle (the primary area of storage for creatine in the body) to fuel anaerobic power activities, thus improving the efficiency of the phosphocreatine energy system (Smith-Ryan & Jose, 2013). Nevertheless, severe adverse effects of Cr are absent in clinical trial studies on Cr, which is a tremendous outcome for a supplement that may enhance performance and lean body mass (Smith-Ryan & Jose, 2013).
A con of Cr is that some individuals are poor or non-responders, which is influenced by the person's genotype (Smith-Ryan & Jose, 2013). Another point to consider is the quality of the product and additional components that make the Cr product less pure.
A practical application to adding Cr monohydrate salt to an athlete's regimen would be to consider starting at 0.3 grams per kilogram of body weight daily post resistance training to improve strength and lean body mass (Smith-Ryan & Jose, 2013). Rawson (2018) indicated two Cr supplementation strategies: short-term ingestion at 20 grams daily for five days or 3-5 grams daily for four weeks to achieve maximal muscle creatine levels. Continuous intake of Cr at a low dose can safely be accomplished at 3-5 grams per day or through dietary sources, which yields about 0.7 grams of creatine per six ounces of meat (Rawson, 2018). Additionally, athletes may consider consuming a post-workout meal or supplement that contains a combination of protein, carbohydrates, and Cr supplement, which has been shown in research to promote greater hypertrophy results than just proteins and carbohydrates alone (Smith-Ryan & Jose, 2013).
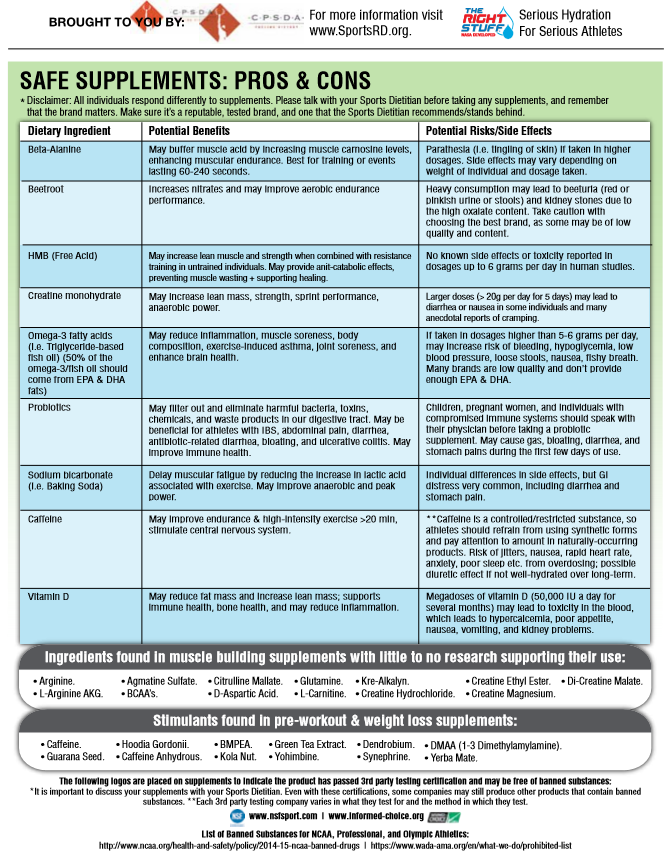
Guidance on Ergogenic Aids
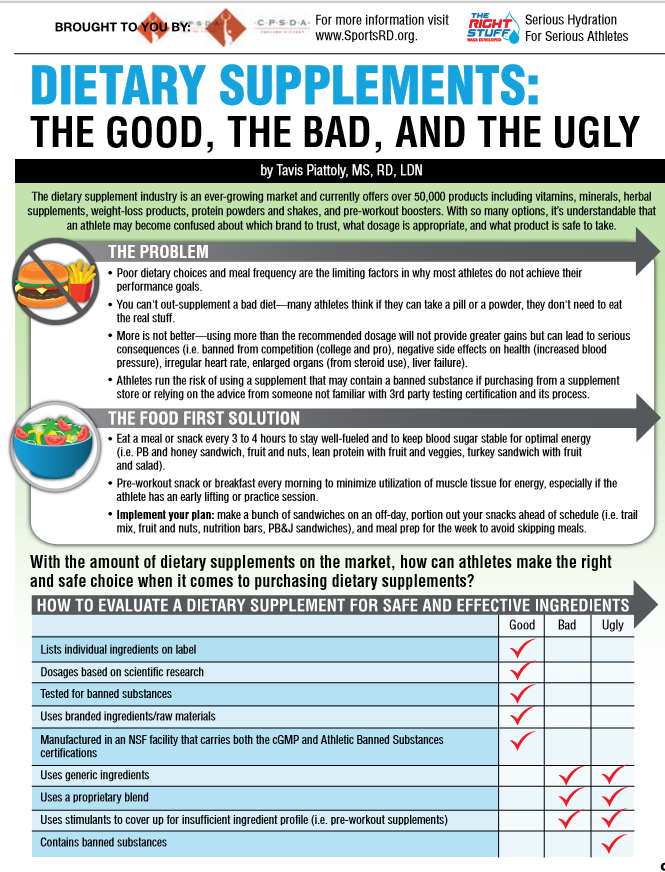
The marketing of supplements does a great job highlighting products and making them look too good to be accurate and allowing the illusion that they may demonstrate erogenic benefits; however, I would encourage all athletes not to fall for the marketing scheme because safety, quality, validity, and effectiveness matter (See Figure 3). Additionally, products may not be approved by governing bodies, and taking a product with hidden additives may place the athlete at risk of falling into a category of doping or illegal substance use. I recommend that every athlete works with a sports dietician familiar with high school and collegiate protocols on supplementation usage.
Figure 1
Stages in the athletic, educational, and nutrition development of the young athlete
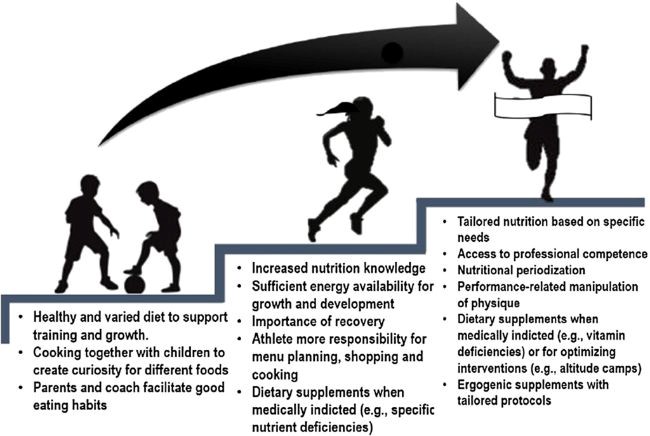
Note. The image was derived from Garthe & Maughan (2018).
Article by Denise Fisher
References
Andersen, L. L., Tufekovic, G., Zebis, M. K., Crameri, R. M., Verlaan, G., Kjær, M., Suetta, C., Magnusson, P., & Aagaard, P. (2005). The effect of resistance training combined with timed ingestion of protein on muscle fiber size and muscle strength. Metabolism, 54(2), 151–156. https://doi.org/10.1016/j.metabol.2004.07.012
Burke, L., Deakin, V., & Minehan, M. (2021). Clinical sports nutrition (6th ed.). McGraw Hill Education Australia.
Burke, L. M. (2017). Practical issues in evidence-based use of performance supplements: Supplement interactions, repeated use and individual responses. Sports Medicine, 47(S1), 79–100. https://doi.org/10.1007/s40279-017-0687-1
Garthe, I., & Maughan, R. J. (2018). Athletes and supplements: Prevalence and perspectives. International Journal of Sport Nutrition and Exercise Metabolism, 28(2), 126–138. https://doi.org/10.1123/ijsnem.2017-0429
Heffernan, S., Horner, K., De Vito, G., & Conway, G. (2019). The role of mineral and trace element supplementation in exercise and athletic performance: A systematic review. Nutrients, 11(3), 696. https://doi.org/10.3390/nu11030696
Jeukendrup, A., & Gleeson, M. (2019). Sport nutrition (3rd ed.). Human Kinetics.
Kerksick, C. M., Wilborn, C. D., Roberts, M. D., Smith-Ryan, A., Kleiner, S. M., Jäger, R., Collins, R., Cooke, M., Davis, J. N., Galvan, E., Greenwood, M., Lowery, L. M., Wildman, R., Antonio, J., & Kreider, R. B. (2018). Issn exercise & sports nutrition review update: Research & recommendations. Journal of the International Society of Sports Nutrition, 15(1). https://doi.org/10.1186/s12970-018-0242-y
Morton, R. W., Murphy, K. T., McKellar, S. R., Schoenfeld, B. J., Henselmans, M., Helms, E., Aragon, A. A., Devries, M. C., Banfield, L., Krieger, J. W., & Phillips, S. M. (2017). A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. British Journal of Sports Medicine, 52(6), 376–384. https://doi.org/10.1136/bjsports-2017-097608
Rawson, E. S. (2018). The safety and efficacy of creatine monohydrate supplementation: What we have learned from the past 25 years of research. Sports Science Exchange, 31(185), 1–6.
Smith-Ryan, A. E., & Jose, A. (2013). Sports nutrition and performance enhancing supplements. Linus Learning.
van Loon, L. J. (2013). Protein ingestion prior to sleep: Potential for optimizing post-exercise recovery. Sports Science Exchange, 26(117), 1–5.
Viribay, A., Burgos, J., Fernández-Landa, J., Seco-Calvo, J., & Mielgo-Ayuso, J. (2020). Effects of arginine supplementation on athletic performance based on energy metabolism: A systematic review and meta-analysis. Nutrients, 12(5), 1300. https://doi.org/10.3390/nu12051300
Figure 2: Periodization and Timing of Macronutrients
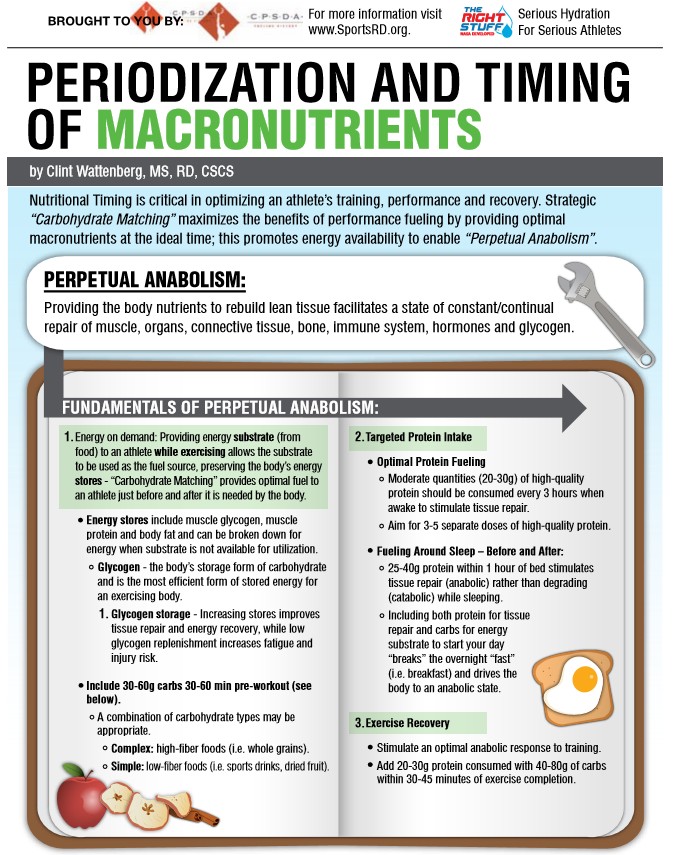
Figure 3: Dietary Supplements

University Hospitals
Sports Nutrition Services for Athletes
Click on the link for more information about UH Sports Nutrition Services for Athletes